Understanding the pharmacokinetics and pharmacodynamics of abiraterone
 Apr, 27 2023
Apr, 27 2023
Introduction to Abiraterone
As a copywriter, I am always eager to learn about new topics and share my knowledge with readers. Today, I want to talk about the pharmacokinetics and pharmacodynamics of abiraterone, a drug that has been making waves in the medical field. Abiraterone is a medication used in the treatment of prostate cancer, specifically metastatic castration-resistant prostate cancer (mCRPC). In this article, we will delve into the intricacies of how abiraterone works in the body, as well as the various factors that affect its efficacy.
The Mechanism of Action of Abiraterone
Abiraterone works by inhibiting the enzyme CYP17A1, which is involved in the synthesis of androgens. Androgens are male hormones that promote the growth of prostate cancer cells. By blocking the production of androgens, abiraterone helps to slow down the progression of prostate cancer. This mechanism of action is what sets abiraterone apart from other prostate cancer treatments, as it targets the root cause of the disease rather than just the symptoms.
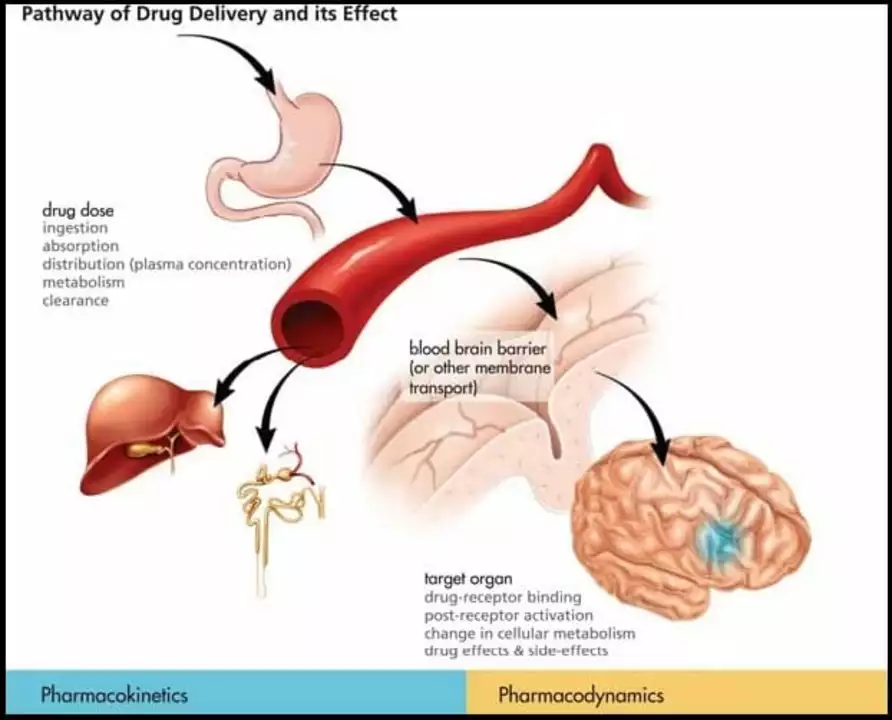
Pharmacokinetics: Absorption, Distribution, Metabolism, and Excretion
Understanding the pharmacokinetics of abiraterone is crucial for healthcare professionals to optimize its use in patients. The pharmacokinetics of a drug refers to how it is absorbed, distributed, metabolized, and excreted by the body. Abiraterone is orally administered and has a high bioavailability, which means that a significant amount of the drug is absorbed into the bloodstream. It is also highly protein-bound, which enables it to be transported to various tissues in the body where it can exert its therapeutic effects.
Abiraterone is primarily metabolized in the liver by enzymes called cytochrome P450 (CYP) 3A4 and 2D6. The metabolites produced in this process are then excreted in the feces and urine. The elimination half-life of abiraterone is approximately 12 hours, which means that it takes about 12 hours for the body to clear half of the drug from the bloodstream. This information is essential for healthcare professionals to determine the appropriate dosing regimen for their patients.
Factors Affecting the Pharmacokinetics of Abiraterone
Several factors can influence the pharmacokinetics of abiraterone, such as age, body weight, liver function, and the presence of other medications. For example, older patients or those with liver impairment may have altered metabolism of the drug, which could potentially lead to increased exposure and a higher risk of side effects. Healthcare professionals must be aware of these factors and adjust the dosing regimen accordingly to ensure the safe and effective use of abiraterone.
Pharmacodynamics: The Relationship Between Drug Concentration and Effect
The pharmacodynamics of a drug refers to the relationship between its concentration in the body and its therapeutic effect. In the case of abiraterone, its pharmacodynamic effect is the inhibition of androgen synthesis, which ultimately leads to a reduction in prostate cancer growth. Understanding the pharmacodynamics of abiraterone is crucial for healthcare professionals to predict the drug's effectiveness and potential side effects in patients.
Factors Affecting the Pharmacodynamics of Abiraterone
Just like the pharmacokinetics, several factors can influence the pharmacodynamics of abiraterone. These factors include the individual patient's sensitivity to the drug, the presence of other medications that may interact with abiraterone, and genetic variations in the enzymes responsible for metabolizing the drug. Healthcare professionals must consider these factors when prescribing abiraterone to ensure the best possible outcome for their patients.
Monitoring the Efficacy and Safety of Abiraterone
Regular monitoring is crucial when administering abiraterone to ensure its efficacy and safety. Healthcare professionals must keep track of the patient's prostate-specific antigen (PSA) levels, which is a biomarker for prostate cancer progression. A decline in PSA levels is usually indicative of a positive response to treatment. Additionally, healthcare professionals should monitor for potential side effects of abiraterone, such as hypertension, hypokalemia, and liver toxicity, and adjust the dosing regimen if necessary.
Conclusion
In conclusion, abiraterone is a groundbreaking medication for the treatment of prostate cancer, specifically mCRPC. Understanding the pharmacokinetics and pharmacodynamics of abiraterone is critical for healthcare professionals to optimize its use in patients and ensure the best possible outcome. By considering factors that can affect the drug's absorption, distribution, metabolism, and excretion, as well as its therapeutic effect, healthcare professionals can tailor the treatment plan to meet the individual needs of each patient.
Emily Kidd
April 28, 2023 AT 18:47caiden gilbert
April 30, 2023 AT 18:46Justin Cheah
May 1, 2023 AT 01:37Aditya Singh
May 1, 2023 AT 19:34shivam mishra
May 3, 2023 AT 03:11Kathy Pilkinton
May 4, 2023 AT 22:37MOLLY SURNO
May 6, 2023 AT 10:23Penny Clark
May 7, 2023 AT 15:42Erin Corcoran
May 7, 2023 AT 16:14Arrieta Larsen
May 9, 2023 AT 12:12Alex Hundert
May 10, 2023 AT 07:55shivam mishra
May 11, 2023 AT 23:01Justin Cheah
May 12, 2023 AT 09:08Mansi Gupta
May 13, 2023 AT 15:14Holly Dorger
May 15, 2023 AT 09:27Jackson Olsen
May 17, 2023 AT 09:06Katherine Reinarz
May 17, 2023 AT 23:48Scott Dill
May 19, 2023 AT 12:29phenter mine
May 20, 2023 AT 18:08Mike Gordon
May 20, 2023 AT 21:51